The quality of bacterial infection serology tests in Germany: Evaluation of the 2020 external quality assurance schemes – a report by the Quality Assurance Commission of the German Society for Hygiene and Microbiology
Ulyana Gräf 1,2Klaus-Peter Hunfeld 1,2,3
Sabine Goseberg 2
1 Institute for Laboratory Medicine, Microbiology and Infection Control, Northwest Medical Centre, Frankfurt am Main, Germany
2 INSTAND e.V., Düsseldorf, Germany
3 German Society for Hygiene and Microbiology (DGHM), Quality Assurance Commission, Hannover, Germany
Abstract
External quality assurance (EQA) tests are used to validate diagnostic testing procedures in the context of quality assurance. They are mandatory and the frequency of participation varies depending on the parameters and whether the test is offered by the laboratory. Samples are analyzed under routine conditions by each EQA test participant and the measurement results are transmitted to the reference institute (Richtlinie der Bundesärztekammer zur Qualitätssicherung laboratoriumsmedizinischer Untersuchungen [guideline of the German Medical Association for the quality assurance of laboratory medical examinations] 2023). The results of the 2020 EQA schemes are presented in more detail below.
Keywords
EQA tests, quality assurance
1 Introduction
External quality assurance (EQA) tests are a way to provide external quality assurance for laboratories. Standardized, validated processes are certified as part of this process [1]. Every laboratory must participate in EQA testing on a regular basis. EQA tests are a means of verifying and comparing the performance and suitability of testing procedures [2].
All laboratories participating in the EQA test receive identical samples. The sample material is usually serum, however, urine can also be used to directly detect pathogens. These samples are analyzed using routine test methods and the results are transmitted to a reference institute within a specified period of time. The aim of bacterial infection serology is to identify the antibodies that have formed after contact with a respective pathogen [3].
This report presents and discusses the results of the 2020 INSTAND EQA schemes for bacterial infection serology.
2 Methods
2.1 Sample collection and implementation
The EQA test samples are obtained from healthy donors or donors who have had a previous infection. Informed consent is obtained from the donors beforehand.
Every laboratory participating in INSTAND e.V.’s EQA schemes receives two serum samples per year to detect specific antibodies against yersinia, bordetella pertussis, mycoplasma, campylobacter and coxiella respectively. All other parameters (including diagnostic inflammatory markers) are tested two to four times a year depending on the participant. For EQA schemes 313 and 316, participants receive two pre-fixed slides and two urine samples that have been spiked with the inactivated cell culture supernatant of a Chlamydia trachomatis culture. The antibody reactivity of the serum samples is blinded for the individual participants. Furthermore, no detailed clinical information is disclosed in order to ensure maximum objectivity with regard to the testing and reporting of the laboratory results. The microbiological stability, sterility and homogeneity of the samples are ensured during production (in accordance with DIN ISO 13528 Annex B) [4], and the samples have tested negative for human immunodeficiency virus (HIV), hepatitis B virus (HBV) and hepatitis C virus (HCV).
2.2 Target values
The target values for the qualitative, semi-quantitative and quantitative test results (if applicable for the EQAs) as well as the comprehensive diagnostic evaluation and the interpretative comments are based on the results of 3 to 10 designated reference laboratories. If a uniform target value for a particular quantitative parameter or analytical method cannot be determined, the robust mean (Algorithm A according to DIN ISO 13528, Annex C) of a collective is used as the target value for a specific test method [4].
With respect to the qualitative test results, either the mode of the results of the reference laboratories or – if a uniform target value for a particular parameter or analytical method cannot be determined – the mode of the results of the participants is set as the target value. The laboratory receives a passing grade if its results correspond to those reported by the reference laboratories. Combinations of results or comments are also accepted where applicable.
Test results are only evaluated if a certain assay or test method is used by more than 8 participants (values obtained with the same method and/or reagent manufacturer combination). Evaluating smaller participant collectives based on a consensus value may lead to statistically invalid assessments in some cases. Therefore, a consensus value is not used to evaluate of a smaller number of participants (n≤8). In such cases, participants only receive a participation certificate.
3 Results
3.1 Tetanus serology (310)
All samples were obtained from healthy, vaccinated individuals. Many participants were not aware that, according to the WHO, anti-toxoid antibody concentrations of between 0.01 and 0.099 IU/mL should be regarded as a positive quantitative test result, even though it does not indicate immune protection [5]. This led to low qualitative pass rates despite excellent, quantitative results and clinical interpretations (pass rates: 73–94%).
3.2 Syphilis serology (311)
The positive sample 32 was obtained from a patient years after a sufficiently treated syphilis infection (titer (modal): Treponema pallidum particle agglutination (TPPA): 1,280, venereal disease research laboratory (VDRL): 1; fluorescent treponemal antibody absorption immunoglobulin M (IgM-FTA-abs) test: <5; enzyme immunoassay (EIA); immunoblot: positive for immunoglobulin G (IgG) and negative for IgM). Even without clinical information, the results clearly point to a past infection. The donor, however, is not suitable for blood donations. Negative sample 31 originated from a healthy blood donor without clinical or serological evidence of a syphilis infection in his medical history. With regard to the clinical comment, only comments or combinations of comments indicating a past infection without the need for further treatment were accepted. Overall, pass rates were more or less similar to those observed during recent surveys. New screening tests (chemiluminescent immunoassay (CLIA), chemiluminescent microparticle immunoassay (CMIA), etc.) could not be evaluated quantitatively this time due to a lack of standardization. Figure 1 [Fig. 1] shows the distribution of the immunoblot bands for sample 32 in the different assays.
Figure 1: Manufacturer-specific distribution of immunoblot bands for sample 32 (IgG)
The positive sample 62 (target values: TPPA: 640, polyvalent enzyme linked immunosorbent assay (ELISA): positive, IgG ELISA: positive, VDRL: 0–2, positive, borderline, negative, FTA-ABS-IgG: 80, positive; FTA-ABS-IgM and IgM-ELISA: negative) was taken from a blood donor with a history of an adequately treated syphilis infection as part of donor screening. For sample 61, which was clearly negative and taken from a healthy blood donor, both the reference laboratories and the participants reported negative test results (overall pass rates for both samples: 83–100%). The overall pass rate for the clinical evaluation was again quite encouraging (82%). Figure 2 [Fig. 2] shows the distribution of the immunoblot bands for sample 62 in the different assays.
Figure 2: Manufacturer-specific distribution of immunoblot bands for sample 62 (IgG)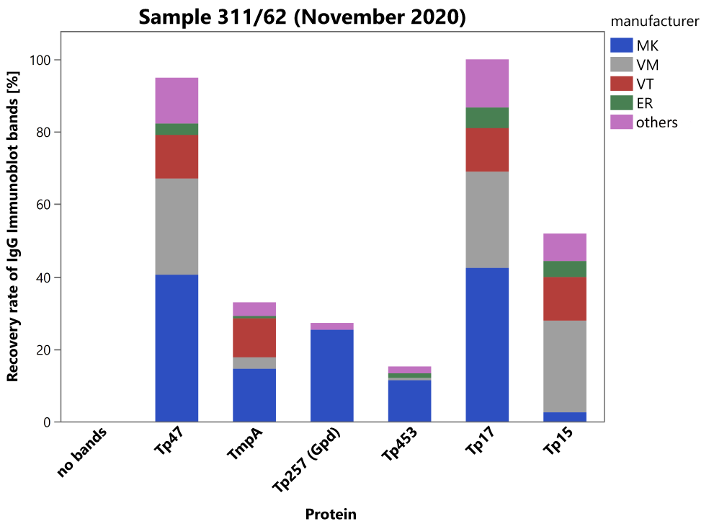
3.3 Chlamydia trachomatis serology (312)
Negative samples 31, 32 and 61 were taken from healthy blood donors with no history of a previous illness. Sample 62 was taken from a PCR-positive patient during the summer months. Weakly positive macrophage migration inhibitory factor(MIF)-IgG (titer: 160), negative MIF-IgM, and weakly positive MIF-IgA (titer: 40) reactivity were found. The assessment “indication of existing or past infection” was accepted. Clinical diagnosis was urethritis! The pass rates for the various methods were predominantly encouraging (clinical comment: 92%; overall pass rates: 75–100%).
3.4 Chlamydia trachomatis (direct detection of Chlamydia antigen (313))
Samples 31 and 62 were produced from sterile urine that tested negative for Chlamydia trachomatis (CT) by polymerase chain reaction (PCR). Samples 32 and 61 were prepared from sterile filtered urine spiked with Chlamydia trachomatis from an inactivated CT culture. The pass rate for negative samples 31 and 62 with no evidence of infection were 73%–100%. The results for the positive samples 32 and 61 were also 73%–100%.
3.5 Chlamydia pneumonia serology (314)
Seronegative samples 31 and 62 were donated by clinically healthy blood donors without symptoms of a respiratory infection in their recent medical history. The seropositive sample 32 was also donated by a clinically healthy blood donor.
Sample 61 was taken from a PCR-positive pneumonia patient in the late summer months. Positive MIF IgG (titer: 640), weakly positive MIF IgM (titer: 80), and positive MIF IgA (titer: 80) reactivity were found, so that only the assessment “no evidence of infection” was accepted. From a clinical and radiological standpoint, there was atypical pneumonia! The pass rates for the various methods were predominantly very encouraging (clinical comment: 74%; overall pass rates: 46–100%) with a relatively clear constellation of findings.
3.6 Yersinia serology (315)
Sample 31 originated from a healthy donor and the serological test result was negative. Sample 32 was obtained from a patient with reactive arthritis and the WIDAL test result was negative even though there was clear reactivity for the immunoglobulin classes IgG, IgM, and IgA in EIA, and immunoblot. The constellation of test results points to a more recent infection and/or yersinia-associated post-infectious sequelae. Again, overall pass rates were encouraging (pass rates: 73–97%).
3.7 Chlamydia trachomatis IFT (316)
In the case of direct C. trachomatis (CT) detection by immune fluorescent testing (IFT), the negative and positive CT samples were fixed on slides before shipment. The slides of negative samples 31 and 62 were coated with non-infected squamous epithelial cells of a urine sediment. For the positive samples 32 and 61, slides were coated with squamous epithelial cells from a urine sediment to which C. trachomatis from a culture supernatant was added. The pass rates ranged between 67% and 83% for both the analytics and the overall diagnostic assessment.
3.8 Bordetella pertussis-serology (317)
Samples 61 and 62 were donated by healthy blood donors without evidence of any recent respiratory infections. Sample 61 tested negative for specific antibodies against B. pertussis and showed no indication of an active or recent infection. Sample 62 showed borderline results for IgG in the ELISA and positive results for IgG in the immunoblot. The sample showed no reactivity for IgA, neither in the ELISA nor in the immunoblot test. The overall pass rates were between 50% and 96%.
3.9 Diphtheria serology (318)
All samples were obtained from healthy, vaccinated individuals. The donors of samples 31 and 62 did not have adequate immune protection and a booster was recommended. From a serological point of view, it can be assumed that the donors of samples 32 and 61 had adequate immune protection. A booster would provide long-term protection. The overall pass rates for the qualitative analysis were 49% to 81%. The pass rates for the quantitative analysis were 79% to 93%.
3.10 Campylobacter serology (319)
Samples 31 and 32 originated from healthy blood donors. Sample 32 showed weakly reactive test results upon IgG testing with ELISA and immunoblot, and a negative test result upon complement fixation testing (CFT) and specific IgM and IgA testing. Some laboratories missed the weak IgG reactivity, leading to pass rates of 77% to 99%.
3.11 Procalcitonin (320)
Samples 31 and 61 were obtained from clinically healthy blood donors. A systemic infection (sepsis) was rather unlikely. Samples 32 and 62 were produced from pooled left-over sera from septic patients and point to a systemic infection (sepsis). The overall pass rates were between 84% and 100%. The pass rates for the interpretative comments ranged between 80% and 88%.
3.12 Streptococcal serology (321)
Samples 31, 61 and 62 came from clinically healthy blood donors. The positive sample 32 was prepared by pooling positive left-over patient sera with the serum of a healthy donor. The pass rates for the different analytical methods used to detect specific antibody concentrations against streptodornase and streptolysin-O ranged from of 78% to 99%.
3.13 Rheumatoid factor (323)
Samples 31 and 61 were obtained from a clinically healthy blood donor. For the positive samples 32 and 62 patient sera that were positive for rheumatoid factor were pooled with the serum of a healthy donor. The overall pass rates ranged between 86% and 99%.
3.14 Mycoplasma pneumonia serology (324)
The seronegative sample 61 was donated by a clinically healthy blood donor whose recent medical history did not indicate any symptoms of an infection. The seropositive sample 62 was also donated by a clinically healthy blood donor. A positive IgG result was obtained by an ELISA test. IgM and IgA showed negative reactivity. The overall pass rates for the different test methods and the interpretative comments were mostly encouraging (overall pass rates: 73% to 100%; interpretative comment: 99%).
3.15 Coxiella burnetii serology (325)
Samples 61 and 62 were donated by healthy blood donors without evidence of a recent infection and tested negative for C. burnetii antibodies. The overall pass rates ranged between 80% and 100%. The pass rate for the interpretative comments was 90%.
3.16 Salmonella serology (331)
Sample 31 was obtained from a healthy blood donor without evidence of a salmonella infection. Sample 32 was prepared from rabbit sera containing high titers of antibodies against Salmonella enterica subsp. enterica, serovar Enteritidis (1, 9, 12: [f], g, m, [p]; [1, 7]) with anti-S. Enteritidis –(O) H titers of 100 (0–400) upon direct agglutination using WIDAL testing. Also, EIA tests to detect human anti-salmonella IgG and IgA antibodies showed weak reactivity for this sample. Accordingly, positive, borderline, and negative WIDAL and EIA test results for this sample were accepted, and medical comments were accepted based on the individual test methods used (over all pass rates: 72–100%).
Sample 61 was taken from a healthy blood donor with no indication of a salmonella infection. Sample 62 was a reactive rabbit antiserum against Salmonella enterica subsp. enterica, serovar Typhi (9, 12, [Vi]: d: –) with anti-S. Typhi –O titers of 400 (100–1,600) in direct agglutination (!) as part of a WIDAL test. Naturally, the ELISA tests designed to detect specific human antibodies had to be negative for this sample, and therefore negative results and assessments were also accepted for these test methods (overall pass rates: 53–100%).
3.17 Borrelia burgdorferi (332)
Sample 31 was donated by a healthy blood donor whose medical history showed no evidence of any tick bites or a manifestation of Lyme disease. Sample 32 also originated from a healthy blood donor but showed isolated moderate reactivity for specific IgG-antibodies against B. burgdorferi in all test systems used throughout the survey. Immunoblot results and banding patterns point to a late phase of the anti-B. burgdorferi immune response. The overall pass rates (67.4–96.2%) and the pass rates for the clinical comments were encouraging (88.1%). The distribution of immunoblot bands reported for the positive sample 32 is depicted in Figure 3 [Fig. 3].
Figure 3: Manufacturer-specific distribution of immunoblot bands for sample 32 (IgG and IgM)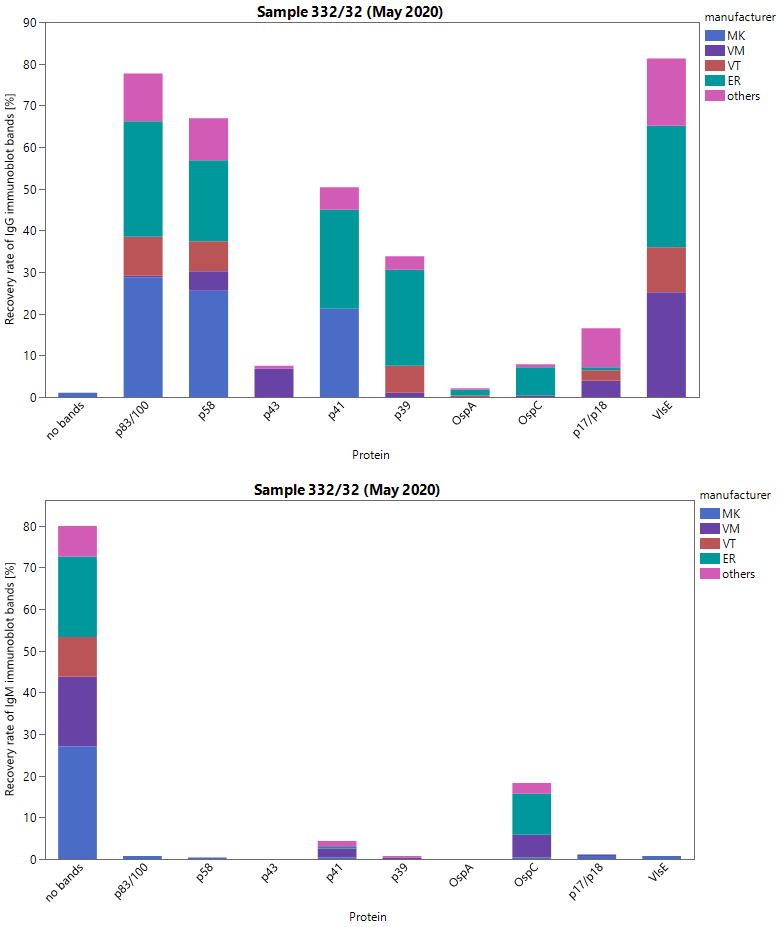
Sample 61 came from a healthy blood donor whose medical history indicated no tick bites or Lyme disease. Sample 62 was taken from a patient who had been successfully treated for erythema migrans approximately one year after treatment of the infection and showed weak specific IgM reactivity in practically all test formats. Regardless of the individual test systems, weakly reactive IgG antibodies were detected with a constellation of findings in the immunoblot that correspond to a late- and an early-stage Borrelia burgdorferi-specific immune response. Both the overall pass rates of the various tests (77–99%) and the clinical evaluation (79%) were relatively encouraging. The distribution of immunoblot bands reported for the positive sample 62 is depicted in Figure 4 [Fig. 4] below.
Figure 4: Manufacturer-specific distribution of immunoblot bands for sample 62 (IgG and IgM)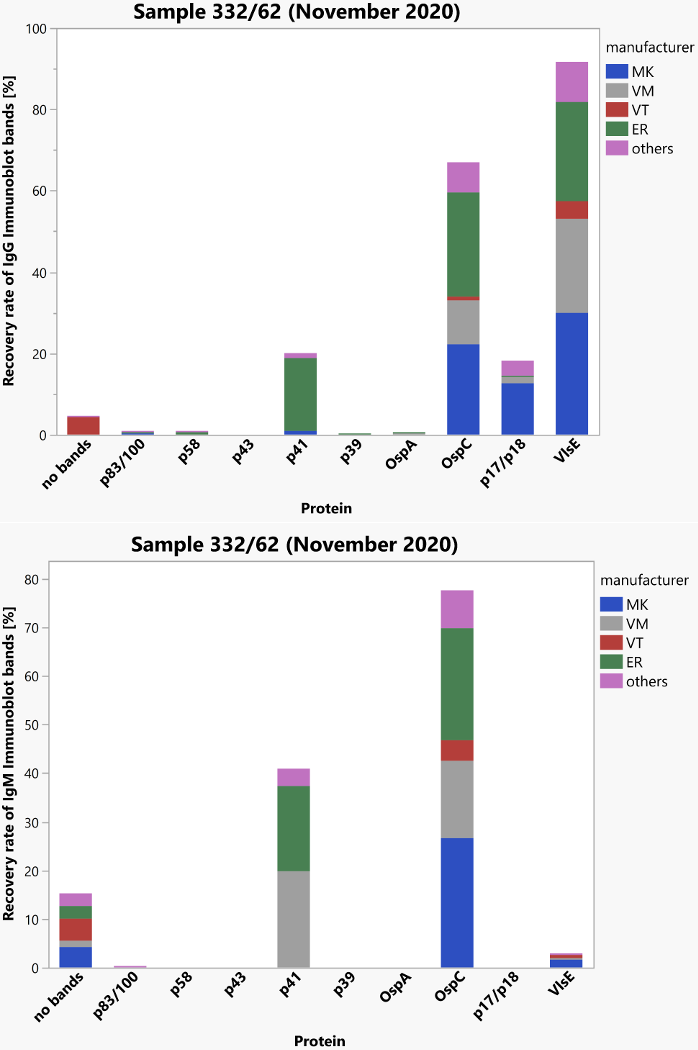
3.18 Helicobacter pylori serology (334)
Negative sample 31 was obtained from a healthy blood donor. Sample 32 also originated from a healthy blood donor and exhibited borderline IgG and IgA antibody reactivity upon EIA and immunoblot testing. Because of the variability of results reported for sample 32, the survey was graded more generously and comments reporting “no infection” as well as comments pointing to a possible infection/colonization were both accepted (overall pass rates: 79–92%).
Negative sample 62 was taken from a healthy blood donor. The positive sample 61, on the other hand, detected positive specific IgG and borderline IgA antibodies with ELISA and immunoblot. It was taken from a Helicobacter-positive patient approximately 1.5 years after completion of the eradication therapy. The participants and the reference laboratories assessed the constellation for sample 62 as a past infection/colonization (overall pass rates: 91–100%).
4 Discussion
The evaluation of the 2020 EQA program for bacterial infections showed that there were few problems except for the fact that the EQA surveys for tetanus and diphtheria conducted in spring 2020 resulted in low qualitative pass rates. Unfortunately, many participants did not consider anti-toxoid antibody test results of between 0.01 and 0.099 IU/ml to be positive. However, according to WHO guidance on anti-toxoid antibody concentrations, these values are considered positive even if there is insufficient immune protection. The quantitative test results and clinical interpretations, on the other hand, were excellent, and the pass rates for most of the other bacterial infection serology schemes examined were excellent and mostly in line with the results of previous EQA surveys.
Notes
Competing interests
The authors declare that they have no competing interests.
References
[1] Bundesärztekammer. Richtlinie der Bundesärztekammer zur Qualitätssicherung laboratoriumsmedizinischer Untersuchungen Gemäß des Beschlusses des Vorstands der Bundesärztekammer in seiner Sitzung am 18.10.2019, zuletzt geändert durch Beschlussfassungen des Vorstands der Bundesärztekammer am 14.04.2023. Dtsch Ärztebl. 2023 May 30;120(21-22). DOI: 10.3238/arztebl.2023.rili_baek_QS_Labor[2] Verordnung über das Errichten, Betreiben und Anwenden von Medizinprodukten (Medizinprodukte-Betreiberverordnung - MPBetreibV), zuletzt geändert durch Art. 7 der Verordnung vom 21. April 2021 (BGBl. I S. 833). § 9 Qualitätssicherungssystem für medizinische Laboratorien.
[3] Rüttger S, Müller I, Hunfeld KP. Zur Qualität bakteriologisch-infektionsserologischer Verfahren in Deutschland: Auswertung der infektionsserologischen Ringversuche 2015 – Beitrag der Qualitätssicherungskommission der DGHM. GMS Z Forder Qualitatssich Med Lab. 2018;9:Doc03. DOI: 10.3205/lab000031
[4] DIN ISO 13528:2020-09: Statistische Verfahren für Eignungsprüfungen durch Ringversuche (ISO 13528:2015, korrigierte Fassung 2016-10-15). Berlin: Beuth; 2020. DOI: 10.31030/3116750
[5] Kuhlmann WD. Tetanus: Impfung, Impftiter und Impfreaktion. Koblenz: Zentrales Institut des Sanitätsdienstes der Bundeswehr; 1991.

