Phimosis and urinary tract infection: An Asian perspective
Shingo Yamamoto 1
1 Department of Urology, Hyogo College of Medicine, Nishinoimiya, Japan
Abstract
Circumcision, the surgical removal of the prepuce, has originally been performed as a ritual procedure among people of certain religions and ethnicities. There are many studies on whether this procedure has advantageous effects on the prevention of urinary tract infection (UTI), mainly from North America and Australia, where circumcision prevalence is between 20 and 80%. Bacterial colonization in the prepuce is documented in literature and could be a legitimate reason why catheterization, but not the bag urine method, is required for uncontaminated urine collection in infants. Circumcision may, but not definitively, reduce the risk of febrile UTI in boys and breakthrough febrile UTI in males with vesicoureteral reflux (VUR). Despite several studies on this topic, there is no prospective study supporting the role of circumcision in patients with VUR to date. Therefore, the guidelines from the American Urological Association and European Association of Urology identified circumcision as an option for UTI prevention. The situation is different in most Asian countries. In Islamic Asian countries, where circumcision rate is nearly 100%, this issue does not raise any clinical concerns. In contrast, circumcision is performed in less than 20% of the males in non-Islamic Asian countries, except for South Korea and the Philippines. In countries where circumcision is not performed during childhood, it is difficult to be conceived as a therapeutic measure by both parents and physicians. The Asian guideline for UTI or sexually transmitted infection, to be published within a year, would advocate recognizing such diversity as a fundamental condition in considering the implication of circumcision in each country. In the future, development and treatment of febrile UTI (fUTI) among uncircumcised boys in these countries should be further studied in a separate context from the countries where circumcision is prevalent.
Abbreviations
AUA: American Urological Association
bUTI: breakthrough urinary tract infection
EAU/ESPU: European Association of Urology/European Society for Paediatric Urology
fUTI: febrile urinary tract infection
STI: sexually transmitted disease
UTI: urinary tract infection
VUR: vesicoureteral reflux
Summary of recommendations
Bacterial flora exists in the inner prepuce, and physicians should be aware that contamination may occur in non-circumcised boys, and catheterization may be required for uncontaminated urine collection (grade of recommendation B; level of evidence 2).
Circumcision may, but not definitively, reduce the risk of fUTI in males and breakthrough febrile UTI in males with VUR. Circumcision should be considered for uncircumcised boys with febrile UTI and VUR in countries where circumcision is accepted among the general population (grade of recommendation B; level of evidence 2), while, in countries where childhood circumcision is rarely performed, other measures for febrile UTI/VUR should be the preferred choice; however, there is insufficient evidence for this problem to date (grade of recommendation C; level of evidence 4).
1 Introduction
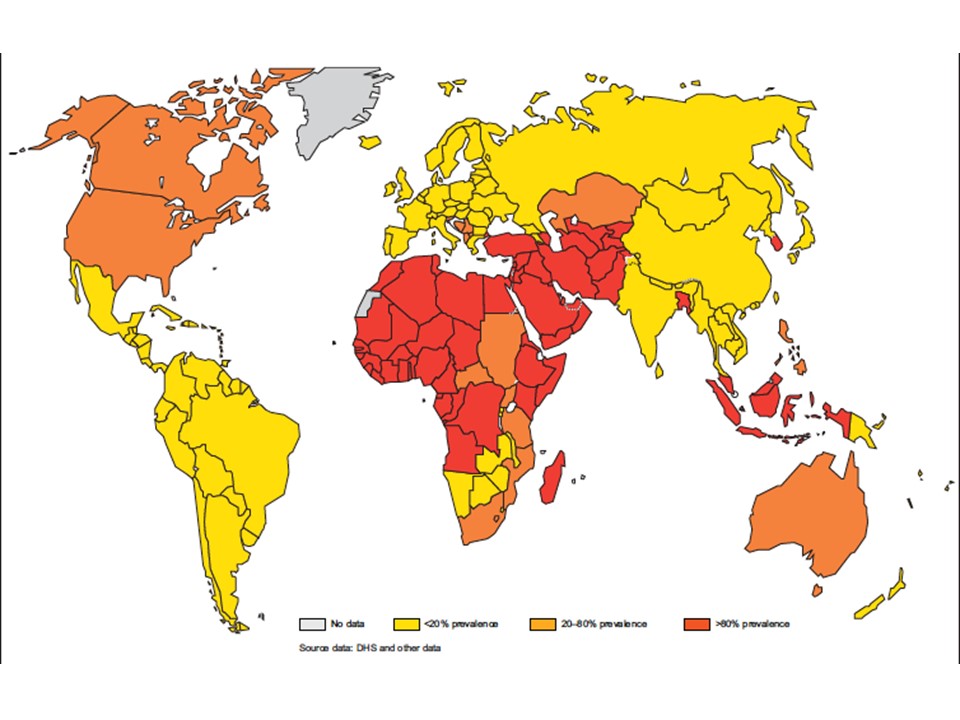
Circumcision, surgical removal of the prepuce, has been performed as a ritual procedure in specific religions and ethnicities, such as Muslim and Jewish people. Many studies have been published to examine whether this originally ritual procedure has an advantageous effect on prevention of urinary tract infection (UTI), especially in male infants with vesicoureteral reflux (VUR). In North America and Australia, where circumcision prevalence is between 20 and 80%, a vital clinical question is whether circumcision should be an option in for treating UTI, and it should be noted that majority of the literature on this topic is from these areas. In contrast, this issue is less frequently mentioned in Asia. In Islamic Asian countries, where the circumcision rate reached nearly 100%, this issue does not raise any clinical problem. In contrast, circumcision is performed in less than 20% of males in non-Islamic Asian countries, except for South Korea and the Philippines (Figure 1) [1]. In countries where neonatal circumcision is routinely performed, no clinical problems may exist in regard to this issue either. In countries where circumcision is not performed during childhood, it is difficult to be conceived as a therapeutic measure by both parents and physicians. In such sense, debates on circumcision arise exclusively from countries where this procedure is performed for some, but not all, male infants.
Because of such radically different socio-ethnical backgrounds in the world, conclusion drawn from studies on one country or ethnicity cannot be equally applied to every other country. At the same time, there are few studies focusing on this topic from Asian and European countries, where circumcision is not frequently performed.
2 Methods
Due to absence of medical literature from countries where circumcision is not frequently performed, the evidence provided in this chapter are inevitably based on literature from countries where circumcision is accepted. The main aim of this chapter was to discuss the applicability of such evidence to Asian populations in a sociocultural context, as described above.
For this purpose, we conducted a PubMed search using a combination of the keywords, “circumcision,” “prepuce,” “urinary tract infection,” “vesicoureteral reflux,” and “children.” The studies were classified into 3 topics:
- preputial bacterial flora,
- UTI, and
- VUR.
Application of these evidences on guidelines in different countries and regions is also discussed.
3 Results
3.1 Preputial bacterial flora and diagnosis of febrile UTI (fUTI) in boys
Colonization of bacteria in the inner prepuce and reduced colonization following circumcision has been documented in studies from the United Kingdom [2], Turkey [3], [4], [5], Israel [6], Ireland [7], and the United States [8]. However, there was one study that reported no difference in bacterial culture between circumcised and uncircumcised males [9] and another study that documented just a modest difference, 37% vs. 28% detection of uropathogenic bacteria, between non-circumcised and circumcised patients with VUR under antibacterial prophylaxis [10]. There are no studies from Asian countries.
Bacterial colonization should be the reason why bag-collected urine from uncircumcised boys produce positive urine culture. This aspect is primarily important in the accuracy of diagnosis of UTI by urine specimen [11]. The American Academy of Pediatrics advocates in its guideline that urine specimen should not be collected by bags but through catheterization [12]. Moreover, it should be noted that the majority of large-scale epidemiological studies related to UTI and circumcision does not specify whether urine specimens were collected by bag or by catheter.
3.2 Circumcision in boys with fUTI
Regarding the prevalence of UTI, there is one prospective randomized study demonstrating the reduction in episode of symptomatic fUTI, but it was not statistically significant [13]. Besides, there have been numerous non-randomized studies reporting decreased fUTI rate in circumcised boys compared with that in non-circumcised boys: cohort studies from Canada [14], Australia [15], and the United States [16], [17], [18] and a series of epidemiological studies from the United States [19], [20], [21], [22]. Three meta-analyses compiling these non-randomized studies were published: two from the United States [22], [23] and one from Australia [24]. There were also two studies comparing the incidences of fUTI before and after circumcision: one from Turkey [25] and one from the United States [26]. However, there are a few studies from areas of Europe and Asia where circumcision is not prevalent.
3.3 Circumcision in boys with VUR
There is no prospective study for the role of circumcision in patients with VUR. One cohort study revealed that, among boys with VUR detected in prenatal hydronephrosis, a higher rate of breakthrough UTI (bUTI) was noted in non-circumcised boys (53%) than circumcised boys (19%) [27]. Another study reported a reduced rate of bUTI after circumcision from 45.2% to 6.2% [28]. There is one report from Japan on the incidence of bUTI during prophylaxis in the non-circumcised population [29]. In comparison to the two reports [27], [28], the percentage of 32.2% of bUTI [29] is lower than the reported percentage in non-circumcised groups but higher than that in circumcised groups. There is another report from Korea on the effect of concomitant circumcision during anti-reflux surgery, which seems not to affect the clinical course [30].
Based on these studies, we may conclude that circumcision reduced the risk of fUTI in males to some extent.
3.4 Guidelines
Circumcision is described as a therapeutic choice for VUR in the American Urological Association guideline of 2010. In the United States, where circumcision rate varies among races but ranges from around 70 to 80% in total, this choice should be presented to parents. The guideline states that, “Although there are insufficient data to evaluate the degree of this increased risk and its duration, parents need to be made aware of this association to permit informed decision-making” [31]. In Europe, the prevalence of circumcision is radically different between countries. Israel and Turkey are at one extreme with nearly 100% prevalence, but majority of countries have less than 20%. In such context, the European Association of Urology/European Society for Paediatric Urology guideline advocates that “Circumcision during early infancy may be considered part of the conservative approach because the procedure has been shown to be effective in reducing the risk of infection in normal children” [32]. Asia has a similar diversity, Muslim Asia and non-Muslim Asia are sharply divided in circumcision prevalence, with exception of South Korea and the Philippines. The Asian guideline for UTI or sexually transmitted infection to be published within a year would advocate recognizing such diversity as a fundamental condition in considering the implication of circumcision in each country.
4 Further research
In countries where neonatal circumcision is routinely performed, no clinical problems may exist in regard to this issue. In countries like Korea and the Philippines where circumcision is performed during childhood, but not as a routine procedure in neonates, one may adopt the conclusions similar to that in the United States and may have the obligation to present circumcision as a choice of treatment in male infants with fUTI and/or VUR.
In countries where circumcision is not routinely performed for children, this procedure may have quite limited role as a treatment for VUR. The natural history of the prepuce was reported in Japan and clearly designated that evolutional history has created human glans to be exposed spontaneously during puberty in almost every man [33]. A Japanese opinion leader, Kenji Shimada, presented his view on this issue stating that “Instead of talking about the negative effect of the prepuce, we have to take lessons from history and reconsider its positive significance” [34]. The word “history” may indicate biological natural history here. Upon such view, in countries where circumcision is not performed during childhood it is difficult to be conceived as a therapeutic measure by both parents and physicians. If the prepuce could be a source of infection, could it be solved by retractablity of the prepuce or is it the presence of the prepuce itself that matters? Such questions deserve further clinical studies in the future.
5 Conclusions
In countries where circumcision is not considered a clinical choice, the association between the prepuce and UTI in men should be reconsidered in a separate context from the literature from countries where circumcision is prevalent. Since there is diversity in the world, there is diversity in clinical practices, as well.
References
[1] World Health Organization. Male circumcision: global trends and determinants of prevalence, safety and acceptability. 2007.[2] Wijesinha SS, Atkins BL, Dudley NE, Tam PK. Does circumcision alter the periurethral bacterial flora? Pediatr Surg Int. 1998 Mar;13(2-3):146-8. DOI: 10.1007/s003830050270
[3] Günşar C, Kurutepe S, Alparslan O, Yilmaz O, Dağlar Z, Sencan A, Genç A, Taneli C, Mir E. The effect of circumcision status on periurethral and glanular bacterial flora. Urol Int. 2004;72(3):212-5. DOI: 10.1159/000077117
[4] Tokgöz H, Polat F, Tan MO, Sipahi B, Sultan N, Bozkirli I. Preputial bacterial colonisation in preschool and primary school children. Int Urol Nephrol. 2005;37(1):101-5. DOI: 10.1007/s11255-004-4700-x
[5] Agartan CA, Kaya DA, Ozturk CE, Gulcan A. Is aerobic preputial flora age dependent? Jpn J Infect Dis. 2005 Oct;58(5):276-8.
[6] Serour F, Samra Z, Kushel Z, Gorenstein A, Dan M. Comparative periurethral bacteriology of uncircumcised and circumcised males. Genitourin Med. 1997 Aug;73(4):288-90. DOI: 10.1136/sti.73.4.288
[7] Glennon J, Ryan PJ, Keane CT, Rees JP. Circumcision and periurethral carriage of Proteus mirabilis in boys. Arch Dis Child. 1988 May;63(5):556-7. DOI: 10.1136/adc.63.5.556
[8] Wiswell TE, Miller GM, Gelston HM Jr, Jones SK, Clemmings AF. Effect of circumcision status on periurethral bacterial flora during the first year of life. J Pediatr. 1988 Sep;113(3):442-6. DOI: 10.1016/S0022-3476(88)80625-5
[9] Hallett RJ, Pead L, Maskell R. Urinary infection in boys: A three-year prospective study. Lancet. 1976 Nov 20;2(7995):1107-10. DOI: 10.1016/S0140-6736(76)91087-4
[10] Cascio S, Colhoun E, Puri P. Bacterial colonization of the prepuce in boys with vesicoureteral reflux who receive antibiotic prophylaxis. J Pediatr. 2001 Jul;139(1):160-2. DOI: 10.1067/mpd.2001.115017
[11] Crain EF, Gershel JC. Urinary tract infections in febrile infants younger than 8 weeks of age. Pediatrics. 1990 Sep;86(3):363-7.
[12] Subcommittee on Urinary Tract Infection, Steering Committee on Quality Improvement and Management; Roberts KB. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011 Sep;128(3):595-610. DOI: 10.1542/peds.2011-1330
[13] Nayir A. Circumcision for the prevention of significant bacteriuria in boys. Pediatr Nephrol. 2001 Dec;16(12):1129-34. DOI: 10.1007/s004670100044
[14] To T, Agha M, Dick PT, Feldman W. Cohort study on circumcision of newborn boys and subsequent risk of urinary-tract infection. Lancet. 1998 Dec 5;352(9143):1813-6. DOI: 10.1016/S0140-6736(98)02392-7
[15] Craig JC, Knight JF, Sureshkumar P, Mantz E, Roy LP. Effect of circumcision on incidence of urinary tract infection in preschool boys. J Pediatr. 1996 Jan;128(1):23-7. DOI: 10.1016/S0022-3476(96)70423-7
[16] Herzog LW. Urinary tract infections and circumcision. A case-control study. Am J Dis Child. 1989 Mar;143(3):348-50. DOI: 10.1001/archpedi.1989.02150150106026
[17] Rushton HG, Majd M. Pyelonephritis in male infants: how important is the foreskin? J Urol. 1992 Aug;148(2 Pt 2):733-6; discussion 737-8. DOI: 10.1016/S0022-5347(17)36706-X
[18] Schoen EJ, Colby CJ, Ray GT. Newborn circumcision decreases incidence and costs of urinary tract infections during the first year of life. Pediatrics. 2000 Apr;105(4 Pt 1):789-93. DOI: 10.1542/peds.105.4.789
[19] Wiswell TE, Smith FR, Bass JW. Decreased incidence of urinary tract infections in circumcised male infants. Pediatrics. 1985 May;75(5):901-3.
[20] Wiswell TE, Roscelli JD. Corroborative evidence for the decreased incidence of urinary tract infections in circumcised male infants. Pediatrics. 1986 Jul;78(1):96-9.
[21] Wiswell TE, Enzenauer RW, Holton ME, Cornish JD, Hankins CT. Declining frequency of circumcision: implications for changes in the absolute incidence and male to female sex ratio of urinary tract infections in early infancy. Pediatrics. 1987 Mar;79(3):338-42.
[22] Wiswell TE, Hachey WE. Urinary tract infections and the uncircumcised state: an update. Clin Pediatr (Phila). 1993 Mar;32(3):130-4. DOI: 10.1177/000992289303200301
[23] Shaikh N, Morone NE, Bost JE, Farrell MH. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008 Apr;27(4):302-8. DOI: 10.1097/INF.0b013e31815e4122
[24] Singh-Grewal D, Macdessi J, Craig J. Circumcision for the prevention of urinary tract infection in boys: a systematic review of randomised trials and observational studies. Arch Dis Child. 2005 Aug;90(8):853-8. DOI: 10.1136/adc.2004.049353
[25] Kose E, Yavascan O, Turan O, Kangin M, Bal A, Alparslan C, Sirin Kose S, Kuyum P, Aksu N. The effect of circumcision on the frequency of urinary tract infection, growth and nutrition status in infants with antenatal hydronephrosis. Ren Fail. 2013;35(10):1365-9. DOI: 10.3109/0886022X.2013.828263
[26] Ginsburg CM, McCracken GH Jr. Urinary tract infections in young infants. Pediatrics. 1982 Apr;69(4):409-12.
[27] Herndon CD, McKenna PH, Kolon TF, Gonzales ET, Baker LA, Docimo SG. A multicenter outcomes analysis of patients with neonatal reflux presenting with prenatal hydronephrosis. J Urol. 1999 Sep;162(3 Pt 2):1203-8. DOI: 10.1016/S0022-5347(01)68134-5
[28] Alsaywid BS, Saleh H, Deshpande A, Howman-Giles R, Smith GH. High grade primary vesicoureteral reflux in boys: long-term results of a prospective cohort study. J Urol. 2010 Oct;184(4 Suppl):1598-603. DOI: 10.1016/j.juro.2010.04.021
[29] Kaneko K, Ohtomo Y, Shimizu T, Yamashiro Y, Yamataka A, Miyano T. Antibiotic prophylaxis by low-dose cefaclor in children with vesicoureteral reflux. Pediatr Nephrol. 2003 May;18(5):468-70. DOI: 10.1007/s00467-003-1111-7
[30] Kwak C, Oh SJ, Lee A, Choi H. Effect of circumcision on urinary tract infection after successful antireflux surgery. BJU Int. 2004 Sep;94(4):627-9. DOI: 10.1111/j.1464-410X.2004.05014.x
[31] Peters CA, Skoog SJ, Arant BS Jr, Copp HL, Elder JS, Hudson RG, Khoury AE, Lorenzo AJ, Pohl HG, Shapiro E, Snodgrass WT, Diaz M. Summary of the AUA Guideline on Management of Primary Vesicoureteral Reflux in Children. J Urol. 2010 Sep;184(3):1134-44. DOI: 10.1016/j.juro.2010.05.065
[32] Stein R, Dogan HS, Hoebeke P, Kočvara R, Nijman RJ, Radmayr C, Tekgül S; European Association of Urology; European Society for Pediatric Urology. Urinary tract infections in children: EAU/ESPU guidelines. Eur Urol. 2015 Mar;67(3):546-58. DOI: 10.1016/j.eururo.2014.11.007
[33] Kayaba H, Tamura H, Kitajima S, Fujiwara Y, Kato T, Kato T. Analysis of shape and retractability of the prepuce in 603 Japanese boys. J Urol. 1996 Nov;156(5):1813-5. DOI: 10.1016/S0022-5347(01)65544-7
[34] Shimada K. Editorial comment to circumcision related to urinary tract infections, sexually transmitted infections, human immunodeficiency virus infections, and penile and cervical cancer. Int J Urol. 2013 Aug;20(8):775-6; discussion 776-7. DOI: 10.1111/iju.12176

